Le rôle évolutif de la TCO dans la myopie pathologique
Résumé
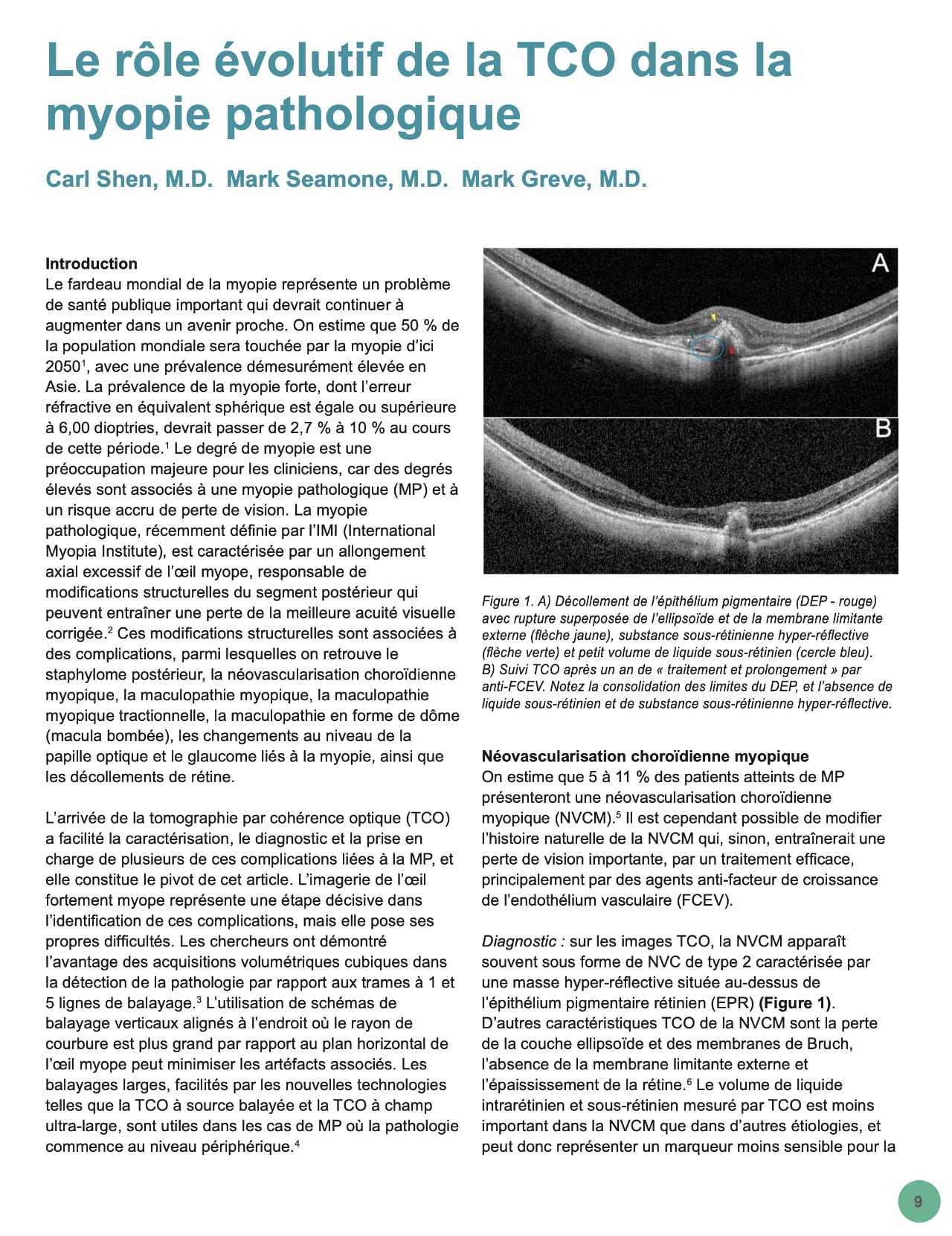
Le fardeau mondial de la myopie représente un problème de santé publique important qui devrait continuer à augmenter dans un avenir proche. On estime que 50 % de la population mondiale sera touchée par la myopie d’ici 2050, avec une prévalence démesurément élevée en Asie. La prévalence de la myopie forte, dont l’erreur réfractive en équivalent sphérique est égale ou supérieure à 6,00 dioptries, devrait passer de 2,7 % à 10 % au cours de cette période. Le degré de myopie est une préoccupation majeure pour les cliniciens, car des degrés élevés sont associés à une myopie pathologique (MP) et à un risque accru de perte de vision. La myopie pathologique, récemment définie par l’IMI (International Myopia Institute), est caractérisée par un allongement axial excessif de l’œil myope, responsable de modifications structurelles du segment postérieur qui peuvent entraîner une perte de la meilleure acuité visuelle corrigée. Ces modifications structurelles sont associées à des complications, parmi lesquelles on retrouve le staphylome postérieur, la néovascularisation choroïdienne myopique, la maculopathie myopique, la maculopathie myopique tractionnelle, la maculopathie en forme de dôme (macula bombée), les changements au niveau de la papille optique et le glaucome liés à la myopie, ainsi que les décollements de rétine.
L’arrivée de la tomographie par cohérence optique (TCO) a facilité la caractérisation, le diagnostic et la prise en charge de plusieurs de ces complications liées à la MP, et elle constitue le pivot de cet article. L’imagerie de l’œil fortement myope représente une étape décisive dans l’identification de ces complications, mais elle pose ses propres difficultés. Les chercheurs ont démontré l’avantage des acquisitions volumétriques cubiques dans la détection de la pathologie par rapport aux trames à 1 et 5 lignes de balayage. L’utilisation de schémas de balayage verticaux alignés à l’endroit où le rayon de courbure est plus grand par rapport au plan horizontal de l’œil myope peut minimiser les artéfacts associés. Les balayages larges, facilités par les nouvelles technologies telles que la TCO à source balayée et la TCO à champ ultra-large, sont utiles dans les cas de MP où la pathologie commence au niveau périphérique.
Références
Holden BA, Fricke TR, Wilson DA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042.
Flitcroft DI, He M, Jonas JB, et al. IMI – Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20-M30.
Sayanagi K, Morimoto Y, Ikuno Y, Tano Y. Spectral-domain optical coherence tomographic findings in myopic foveoschisis. Retina. 2010;30(4):623-628.
Ohno-Matsui K, Fang Y, Shinohara K, Takahashi H, Uramoto K, Yokoi T. Imaging of Pathologic Myopia. Asia-Pacific J Ophthalmol (Philadelphia, Pa). 2019;8(2):172-177.
Wong TY, Ferreira A, Hughes R, Carter G, Mitchell P. Epidemiology and disease burden of pathologic myopia and myopic choroidal neovascularization: an evidence-based systematic review. Am J Ophthalmol. 2014;157(1).
Milani P, Pece A, Pierro L, Bergamini F. Imaging of naive myopic choroidal neovascularization by spectral-domain optical coherence tomography. Ophthalmologica. 2014;232(1):28-36.
Lai TYY, Cheung CMG. Myopic Choroidal Neovascularization: Diagnosis and Treatment. Retina. 2016;36(9):1614-1621.
Zicarelli F, Azzolini C, Cornish E, et al. Optical coherence tomography features of choroidal neovascularization and their correlation with age, gender, and underlying disease. Retina. 2021;41(5):1076-1083.
Leveziel N, Caillaux V, Bastuji-Garin S, Zmuda M, Souied EH. Angiographic and optical coherence tomography characteristics of recent myopic choroidal neovascularization. Am J Ophthalmol. 2013;155(5):913- 919.
Iacono P, Giorno P, Varano M, Parravano M. Structural and optical coherence tomography angiography in myopic choroidal neovascularization: Agreement with conventional fluorescein angiography. Eur J Ophthalmol. 2021;31(1):149-157.
Miyata M, Ooto S, Hata M, et al. Detection of Myopic Choroidal Neovascularization Using Optical Coherence Tomography Angiography. Am J Ophthalmol. 2016;165:108-114.
Battista M, Sacconi R, Borrelli E, et al. Discerning Between Macular Hemorrhages Due to Macular Neovascularization or Due to Spontaneous Bruch’s Membrane Rupture in High Myopia: A Comparative Analysis Between OCTA and Fluorescein Angiography. Ophthalmol Ther. 2022;11(2):821-831.
Introini U, Casalino G, Querques G, Gimeno AT, Scotti F, Bandello F. Spectral-domain OCT in anti-VEGF treatment of myopic choroidal neovascularization. Eye (Lond). 2012;26(7):976-982.
Bruyère E, Caillaux V, Cohen SY, et al. Spectral-Domain Optical Coherence Tomography of Subretinal Hyperreflective Exudation in Myopic Choroidal Neovascularization. Am J Ophthalmol. 2015;160(4):749-758.e1.
Ikuno Y, Jo Y, Hamasaki T, Tano Y. Ocular risk factors for choroidal neovascularization in pathologic myopia. Invest Ophthalmol Vis Sci. 2010;51(7):3721-3725.
Ahn SJ, Park KH, Woo SJ. Subfoveal Choroidal Thickness Changes Following Anti-Vascular Endothelial Growth Factor Therapy in Myopic Choroidal Neovascularization. Invest Ophthalmol Vis Sci. 2015;56(10):5794-5800.
Panozzo G, Mercanti A. Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol (Chicago, Ill 1960). 2004;122(10):1455-1460.
Parolini B, Palmieri M, Finzi A, et al. The new Myopic Traction Maculopathy Staging System. Eur J Ophthalmol. 2021;31(3):1299-1312.
Shimada N, Tanaka Y, Tokoro T, Ohno-Matsui K. Natural course of myopic traction maculopathy and factors associated with progression or resolution. Am J Ophthalmol. 2013;156(5).
Ripandelli G, Rossi T, Scarinci F, Scassa C, Parisi V, Stirpe M. Macular vitreoretinal interface abnormalities in highly myopic eyes with posterior staphyloma: 5-year follow-up. Retina. 2012;32(8):1531-1538.
Jo Y, Ikuno Y, Nishida K. Retinoschisis: a predictive factor in vitrectomy for macular holes without retinal detachment in highly myopic eyes. Br J Ophthalmol. 2012;96(2):197-200.
Sborgia G, Boscia F, Niro A, et al. Morphologic and functional outcomes of different optical coherence tomography patterns of myopic foveoschisis after vitrectomy and inner limiting membrane peeling. Eye (Lond). 2019;33(11):1768-1775.
Grewal PS, Lapere SRJ, Gupta RR, Greve M. Macular buckle without vitrectomy for myopic macular schisis: a Canadian case series. Can J Ophthalmol. 2019;54(1):60-64.
Alkabes M, Mateo C. Macular buckle technique in myopic traction maculopathy: a 16-year review of the literature and a comparison with vitreous surgery. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):863- 877.
Grewal PS, Seamone M, Greve M, Deveau A, Gupta RR. Internal Chandelier-Assisted Macular Buckling for Myopic Foveoschisis. Retin Cases Brief Rep. 2020;Publish Ah.
Bruyère E, Philippakis E, Dupas B, Nguyen-Kim P, Tadayoni R, Couturier A. Benefit of interoperative optical coherence tomography for vitreomacular surgery in highly myopic eyes. Retina. 2018;38(10):2035-2044.
Parolini B, Palmieri M, Finzi A, Frisina R. Proposal for the management of myopic traction maculopathy based on the new MTM staging system. Eur J Ophthalmol. 2021;31(6):3265-3276.
Ohno-Matsui K, Kawasaki R, Jonas JB, et al. International photographic classification and grading system for myopic maculopathy. Am J Ophthalmol. 2015;159(5):877-883.e7.
Fang Y, Yokoi T, Nagaoka N, et al. Progression of Myopic Maculopathy during 18-Year Follow-up. Ophthalmology. 2018;125(6):863- 877.
Fang Y, Du R, Nagaoka N, et al. OCT-Based Diagnostic Criteria for Different Stages of Myopic Maculopathy. Ophthalmology. 2019;126(7):1018-1032.
Publié
Comment citer
Numéro
Rubrique
Licence
© Canadian Eye Care Today 2022

Cette œuvre est sous licence Creative Commons Attribution - Pas d'Utilisation Commerciale - Pas de Modification 4.0 International.